Magnetic resonance imaging ( MRI) is base don the absorption
and emission of radiofrequency energy by protons whose spin is influenced by
changing magnetic fields ( 0.3 to 1.5 T). Unlike computed tomograohy (CT),
there is no radiation exposure.
T1-weighted images cause fat( eg, myelin in the white
matter) to appear bright and wáter( eg, cerebrospinal fluid [CSF] or edema) to
appear dark on this sequence. The gray –white interfaces of the brain are well
depicted on these sequences, esencially if with the images are thinly sliced.



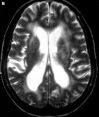
T2-weighted images cause wáter ( eg,CSF and edema) to appear
bright and fat to appear dark.

The MRI-based intravenous contrast agents ( eg, gadolinium)
are frequently used in T1-weight images to make serum appear bright. The
blood-brain barrier typically serves to limit the passage of many molecules out
of the blood vessels. If the disease processes break down this barrier ( such
as infection, tumors,or inflammation), intravenous contrast agents can cross
into the brain, causing áreas of contrast entry to appear very bright.

MRI vs CT
CT can be performed quickly and is preferred in cases of trauma and emergency circunstances. CT is more sensitive for detecting calcification and better delineates cortical bone. CT angiography has better resolution compared with magnetic resonance angiography; however, the latter has the advantage of not absolutely requiring the use of contrast agents. MRI cannot be performed in claustrophobic patients and those with ferromagnetic medical devices, such as pacemakers.Futher, MRI takes longer to perform and might require sedation, precluding its use in emergency situations. However, for evaluating posterior fossa disease, white matter disease, temporal lobe epilepsy, and vascular diseases, MRI is preferable to CT.
Apart from sparing the effect of radiation; mRI is superior to CT in delinesting extent, spread, mass effect, vascularity, necrosis, and edema. T2-weighted sequences are sensitive for detection of tumor and edema.
MRI is superior to CT when there is suspicion of intracranial extension, optic nerve involvement, and cavernous sinus thrombosis because MRI is better for discerning soft tissue disease. Gadolinium is a paramagnetic contrast agent that prolongs the spin of water protons, resulting in postcontrast enhancement of areas of inflammation on T1-weighted imaging. The most sensitive technique for demonstrating orbital infection is post gadolinium fat suppressed T1-weight imaging.
FLAIR is an extremely useful technique in brain imaging. Like conventional T2_weighted imaging, edema appears bright, but this technique nulls ( or makes dark) CSF signal. FLAIR is a sensitive technique for displaying demyelination within the brain, thus clearly revealing lesions in proximity to CSF, such as periventricular plaques in multiple sclerosis. The technique is accomplished via a relatively long inversion time to allow the longitudinal magnetization of CSF to return tl the null point preceding the conventional spin echo imaging. It also has a tremendous role in early detection of cortical gray matter infarcts.The cortical gray matter is vulnerable to ischemia because of its high metabolic activity. However, cortical gray matter immediately adjacent to CSF within the sulci makes infarction hard to delineate when this area undergoes conventional imaging sequences that emphasize fluid signal. FLAIR suppress the CSF signal and makes the cortical or periventricular area more conspicuous.
DWI (Diffusion-weighted imaging) was performed by adding 2 strong diffusion-sensitizing magnetic field gradient pulses. DWI depicts recently infarcted brain as very bright signal. The actual diffusion in the tissue is decreased as seen on apparent diffusion can last 5 to 10 days ( but sometimes less) in pediatric population. DWI can detect ischemic stroke within minutes, in contrast to conventional MRI and can distinguish new and old strokes and acute and
chronic ones. Because abscesses, parenchymal contusions, and cysts can also demonstrate restricted diffusion, DWI also helps detect brain abscesses and cystic tumors.
Magnetic resonance spectroscopy monitors biochemical changes in brain tumors, head trauma, stroke, epilepsy, metabolic disorders, and infections. The metabolites predominantly measured are N-acetylaspartato (NAA), creatine, choline, and myoinositol. NAA, an amino acid found exclusively in neurons, is regarded as a nonspecific marker of neuronal viability. NAA levels are decreased in conditions such as infarction and neuronal inflammation. Lactate is absent in normal brain tissue, and its presence is indicative of anaerobic glycolisis at cellular level. Elevated lactate levels are associated with ischemia or metabolic disorders ( with predominant anaerobic glycolisis). An elevated choline-creatine ratio is suggestive of malignancy. Choline is involved in the synthesis of phospholipid cell membranes; in aggressive neoplasms, choline is elevated because of rapid cell turnover.
Pediatrics in Review
Vol.35 No.3 pp.106-111 March 2014 ( esta en biblioteca en la parte de atrás, revistas nuevas)
chronic ones. Because abscesses, parenchymal contusions, and cysts can also demonstrate restricted diffusion, DWI also helps detect brain abscesses and cystic tumors.
Magnetic resonance spectroscopy monitors biochemical changes in brain tumors, head trauma, stroke, epilepsy, metabolic disorders, and infections. The metabolites predominantly measured are N-acetylaspartato (NAA), creatine, choline, and myoinositol. NAA, an amino acid found exclusively in neurons, is regarded as a nonspecific marker of neuronal viability. NAA levels are decreased in conditions such as infarction and neuronal inflammation. Lactate is absent in normal brain tissue, and its presence is indicative of anaerobic glycolisis at cellular level. Elevated lactate levels are associated with ischemia or metabolic disorders ( with predominant anaerobic glycolisis). An elevated choline-creatine ratio is suggestive of malignancy. Choline is involved in the synthesis of phospholipid cell membranes; in aggressive neoplasms, choline is elevated because of rapid cell turnover.
Pediatrics in Review
Vol.35 No.3 pp.106-111 March 2014 ( esta en biblioteca en la parte de atrás, revistas nuevas)
Me parece muy buen resumen y están excelentes las comparaciones con la CT
ResponderEliminarme gusto la comparación entre ambas técnicas
ResponderEliminarTabla comparativa del libro Adams para complementar el tema
ResponderEliminarhttp://0-accessmedicine.mhmedical.com.millenium.itesm.mx/ViewLarge.aspx?figid=45424713
Muchas gracias, Annie!
EliminarArtículo de complemento
ResponderEliminarhttp://med.javeriana.edu.co/publi/vniversitas/serial/v52n3/4.pdf
Creo que complementa muy bien con lo que viene en el libro acerca de diagnóstico
ResponderEliminarYo encontre este video de resonancia magnetica, ya le entendi mejor!!
ResponderEliminarhttps://www.youtube.com/watch?v=UeJdjw2VZkE
Alejandro Gutierrez C
EliminarA01095635
Martes-Viernes
Esta ppt tambien eta padre:
Eliminarhttp://www.slideshare.net/llueveenparis/resonancia-magntica-12970285
Por si a alguien le interesa http://www.mayoclinic.org/tests-procedures/mri/multimedia/mri/vid-20084743 en este video se explican cosas mas técnicas de este examen :)
ResponderEliminarCreo que está súper bien explicado, y las imágenes ayudan mucho a tener un entendimiento más completo
ResponderEliminarLa información me pareció muy completa y concreta, solo la de la técnica de flair no se me hizo muy clara.
ResponderEliminarMe gusto mucho la explicación de T1 y t2, las imágenes muy buenas
ResponderEliminarExcelente información, me pareció muy completa
ResponderEliminar